Cross Infection Control
Vaccines and Vaccination

Vaccination is also known as immunisation.
Once the immune system has been primed (by the vaccine) to recognise the disease, future infections will be dealt with swiftly by killing the infectious agent (bacteria or virus), before it has a chance to spread and make the person ill.
There are some diseases for which immunisation is not (currently) possible, but many vaccines exist.
Can you name six infectious diseases for which vaccines have been developed?
Can you name two infectious diseases of relevance to the dental team for which there is no vaccine?
Vaccine types
There are many types of vaccine. Sometimes the same disease can have different types of vaccine available. For interested members, further information on the four main types is given below:
Attenuated Vaccine
Inactivated Vaccine
Virus-like particle vaccines
Subunit vaccine
If an individual is immune to an infectious disease, they don’t have to worry about it. If most of the population is immune, the pathogen has nowhere to live, and will die out. Vaccination programmes have eradicated smallpox, and the World Health Organisation is trying to do the same with polio.
Vaccination and dentistry
All members of the dental team should, at a minimum, be vaccinated against TB and hepatitis B. This is for their own protection, and also to ensure they don’t become carriers, and potentially pass the disease on the patients and other staff.
Carrier testing
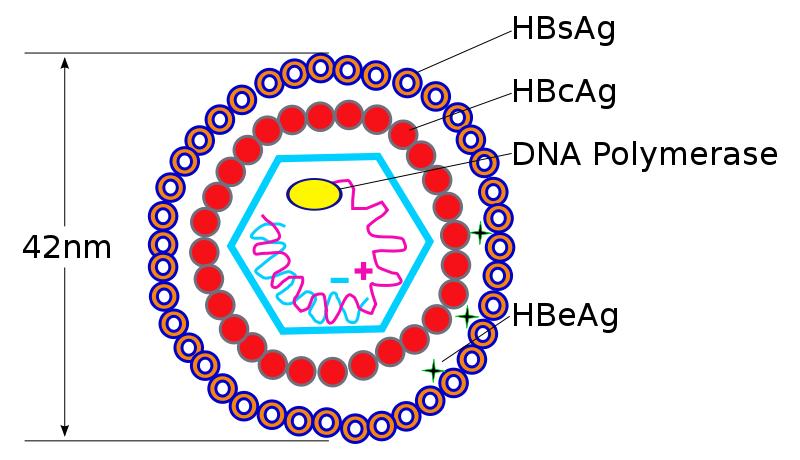
Dental surgery staff should not be an "infection hazard" - that is, they should not be carrying the Hep B virus. The first test for new staff is to see whether they are a carrier.
This is done with a Hepatitis B Surface Antigen test. If they are Antigen Positive, they might be carriers. Further tests on the amount of virus in their blood will determine whether this is the case. If they are carriers, they must not work directly with patients or instruments (i.e. undertake "exposure-prone procedures").
Immunity testing
However, let's hope they are not carriers, and they pass the test.
The next test is to check their immunity to Hepatitis B.
This is done with a Hepatitis B Surface Antibody test. If the antibody levels are high, they are immune, and can work unrestricted. They will be advised (usually by the unit that arranged the testing) how often they should have a booster.
If they have low (or zero) antibodies they will be advised on whether they simply need a booster, or an entire course of immunisation.
Failed immunity
The Hepatitis B vaccination does not work on everyone. If a healthy employee fails to become immune, a decision has to be made:
A) Should they be prevented from exposure-prone procedures, because of the risk to themselves?
B) Should they be allowed to work normally?
Most organisations go for (B), with the proviso that they are tested every three months to ensure they haven't become infected. However, this depends on local guidelines and policies.
Monitoring (and audit) of immune status
It is essential that details of staff immunity are recorded, with original proof of vaccination certificates, and blood test results when appropriate.
There must be a mechanism that reminds staff when they need a booster, and ensures that this gets done.
This log forms part of a practice's Clinical Governance Portfolio. It can be paper based, or computerised.
The log is a confidential practice record: staff confidentiality must be ensured.