Diagnosis
Pathology and Radiology of Dentine Caries
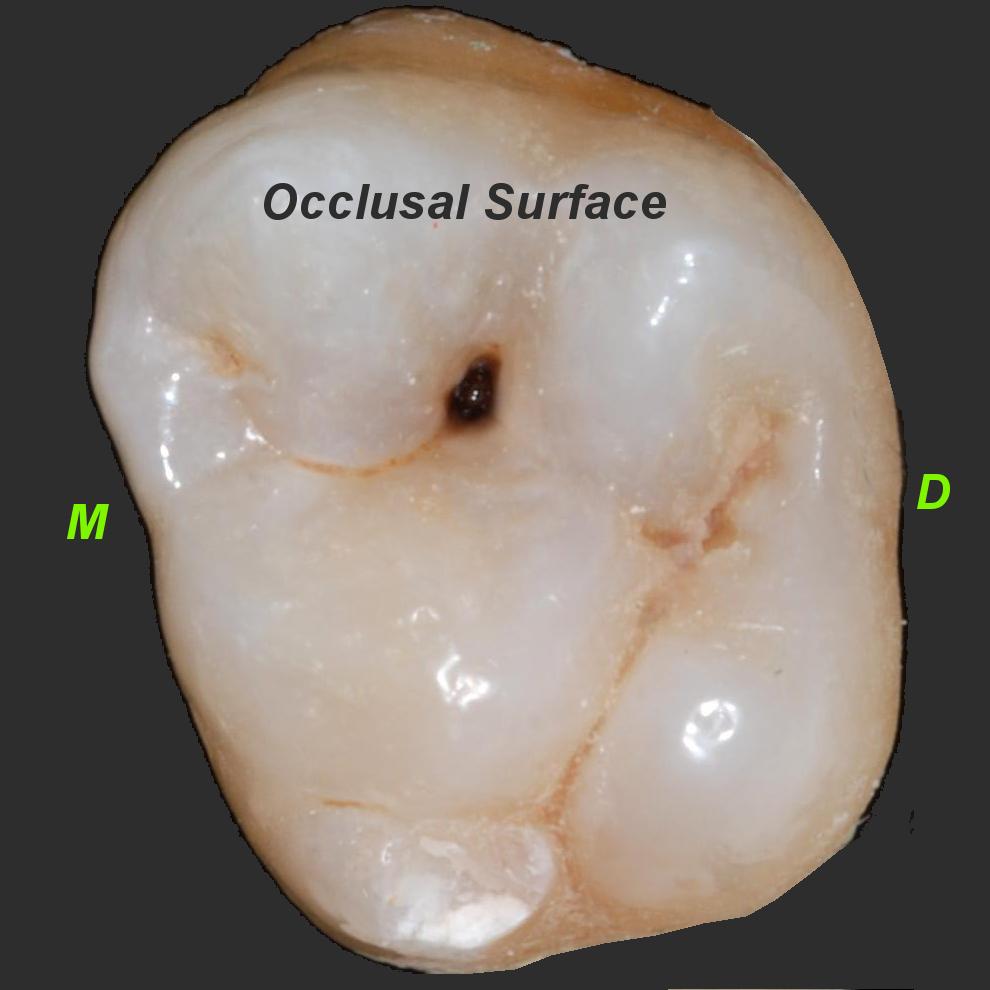
Here is a radiograph of a tooth which shows some radiolucency distally (to the right). Next to it is an occlusal view.
You can magnify many of the pictures on this page by clicking them - look for the icon at the picture bottom-right.

On this evidence alone, would you restore the tooth, or apply preventive measures such as topical fluoride, Diet Advice, and Oral Hygiene Instruction?
What instrument might be helpful in determining if there is a cavity here, and why?

Zones of Dentine Caries
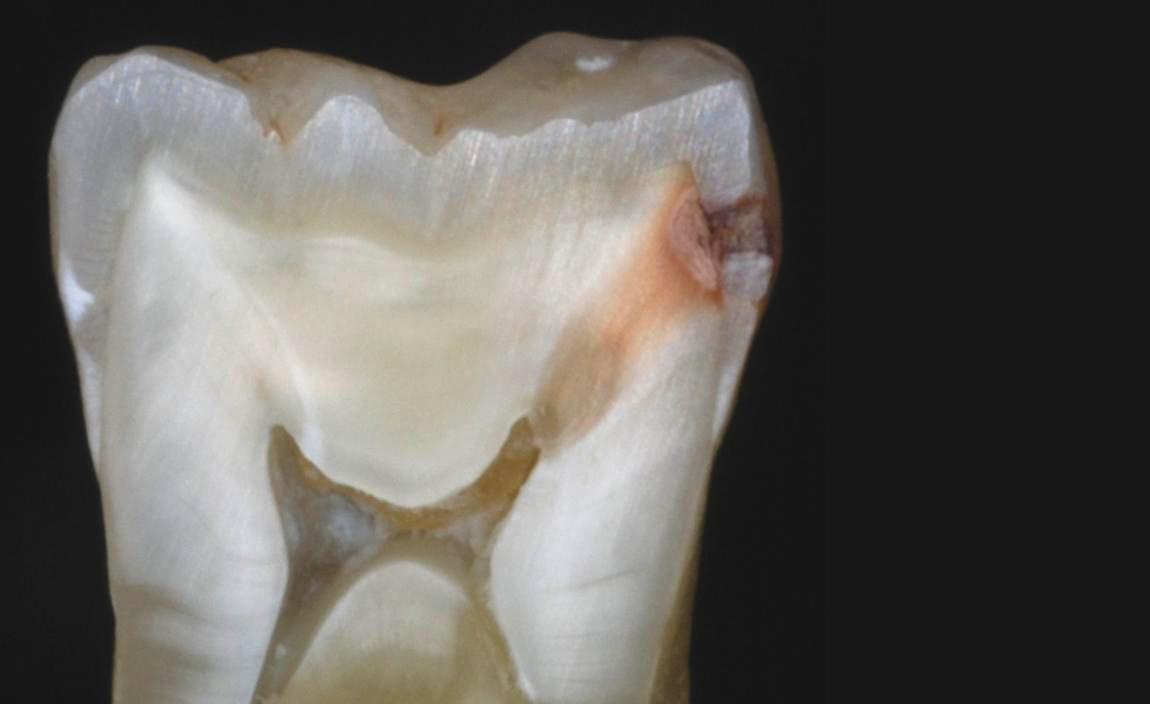
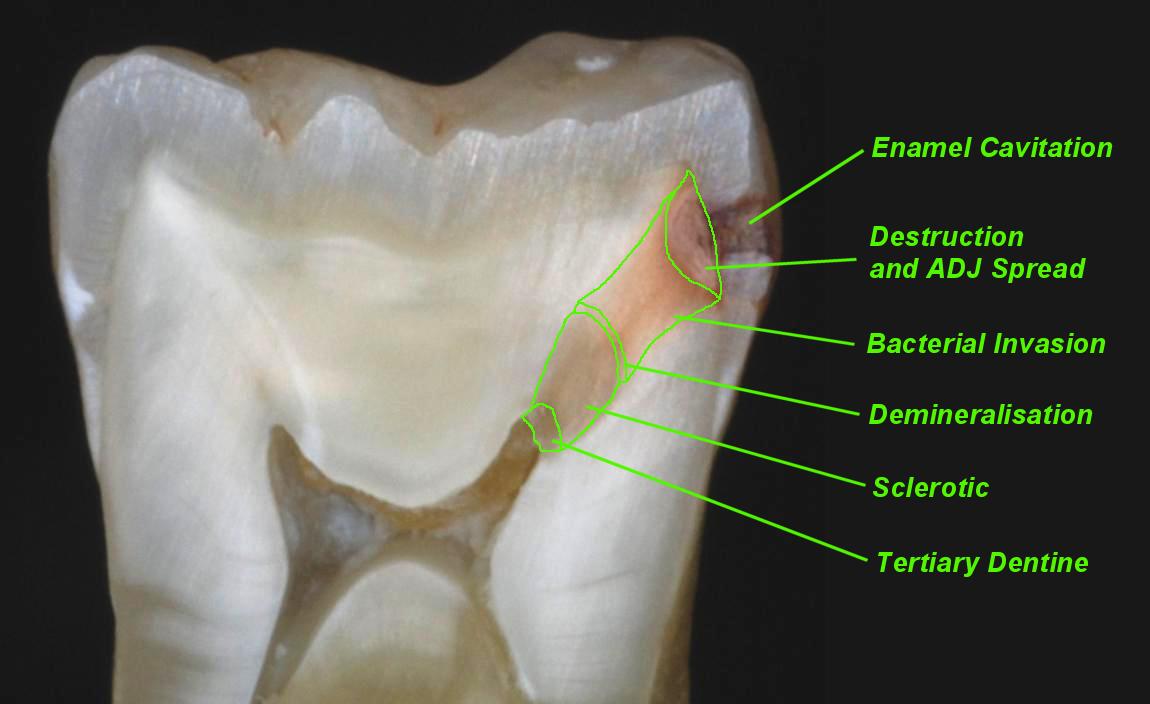
Below is a ground section through the tooth. It shows enamel cavitation, and five Zones of Dentine Caries:
• Zone of destruction
• Zone of Bacterial Invasion
• Zone of Demineralisation
• Sclerotic Zone (also known as Translucent Zone)
• Tertiary Dentine (also known as Reactive Dentine)
Can you identify the area covered by each of the Zones?
Zone of Destruction
When enamel has been cavitated, bacteria infect the dentine. There may be a Zone of Destruction within the dentine, where the dentine becomes necrotic, and liquifies. Cracks appear in the dentine, usually at right angles to the direction of the dentinal tubules. The liquified areas are called Liquefaction Foci, and the cracks are called Transverse Clefts.
With rapid caries, this zone is soft and yellow. With slowly progressing caries, it is harder and browner. This region is easily removed with an excavator.
Zone of Bacterial Invasion
The tubules are invaded by bacteria, which then multiply within the tubule lumen. As well as decalcifying the dentine with acid, the bacteria dissolve the proteins (like collagen) within the tubules. This is called proteolysis. This region can be removed by a rose-head bur, gentle pressure running slowly.
Zone of Demineralisation
Acid produced by the bacteria travels down the dentinal tubules, causing demineralisation. The zone of demineralisation is the advancing front of the carious lesion, and may be very small (less than 1mm). Dentine is relatively easily dissolved/demineralised by acid, at pH 6.7. It is important to note that there are no bacteria in this region.
Clinically, it is very difficult to tell by feel or appearance where the Zone of Bacterial Invasion stops, and the Zone of Demineralisation starts. However, Caries-Indicator Dyes will show which zone you are in.
Sclerotic (Translucent) Zone
A defence reaction occurs within the tubules when acid initially starts to penetrate them. The (live) odontoblast processes start to lay down calcification within the tubules, and they become plugged with mineral deposits. This helps to slow down the acid advance, giving the pulp some protection from the acid.
Occasionally this zone of tubular sclerosis can be seen on radiographs as a radio-dense (whiter) area below the caries, because of the extra mineralisation.
Tertiary Dentine (Reactive Dentine)
When the pulp is mildly inflamed by advancing acid, it produces tertiary dentine in an attempt to wall off the insult.
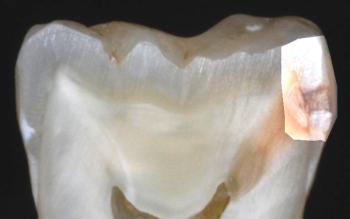
Finally, here is a picture of the distal lesion itself. Although the radiograph didn't show much, cavitation is clearly visible (click to magnify). Note the cavity is below the contact point, so accessible to a contra-angled probe.

How much to remove?
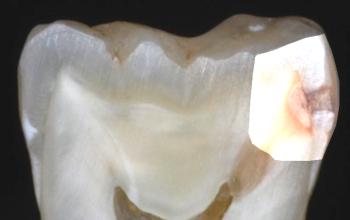
Traditionally, when preparing a cavity for restoration, dentists would (attempt to) remove the Zone of Destruction and the Zone of Bacterial Invasion, rendering the cavity free of bacteria before filling it. Work by Edwina Kidd and others suggests that this may not always be necessary: if the infected zone is well sealed - or entombed - by a restoration, caries progression will halt. However, if the seal should fail in years to come, it will rapidly re-start.
If you adopt this "seal and monitor" philosophy, you must also make a clinical decision about whether to remove the Zone of Destruction: in stress-bearing situations restorative materials need to sit on firm dentine. If the restoration is not stress bearing (for example buccal caries), leaving part of the Zone of Destruction may be justifiable.
Please note that the "seal and monitor" approach requires very careful patient selection if it is to succeed.
|
|
|
| "Classical" preparation removes all infected dentine. Overlying enamel is removed for access. |
"Seal and monitor" preparation just removes Zone of Destruction for this stress bearing situation. |
More Clinical Examples
Have a look at these pictures (click to magnify). Try to decide where the zones are. Do they need operative restoration? How much preparation you would do prior to restoration? Do the radiographs accurately reflect the position and extent of the decay?
The zones to look for are -
• Zone of destruction
• Zone of Bacterial Invasion
• Zone of Demineralisation
• Sclerotic Zone
• Tertiary Dentine
| Occlusal caries, ADJ spread. | 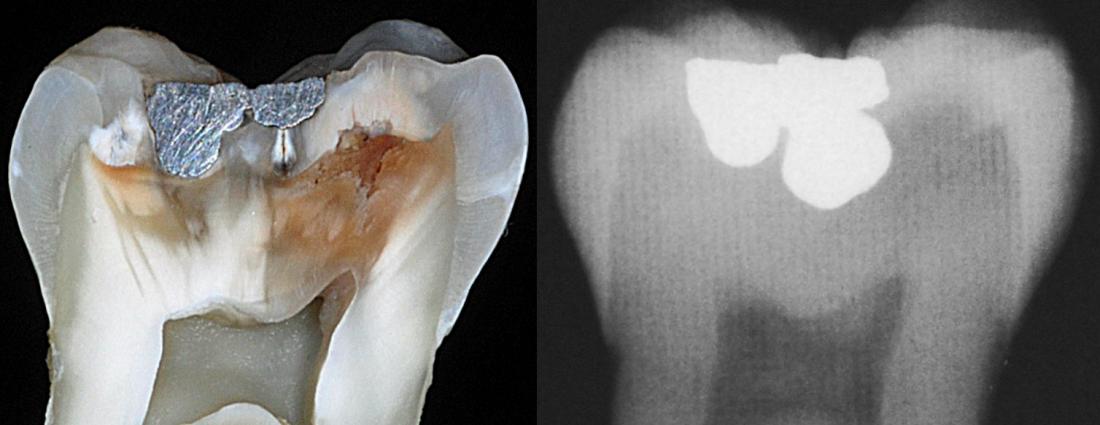 |
| Mesial and occlusal caries | 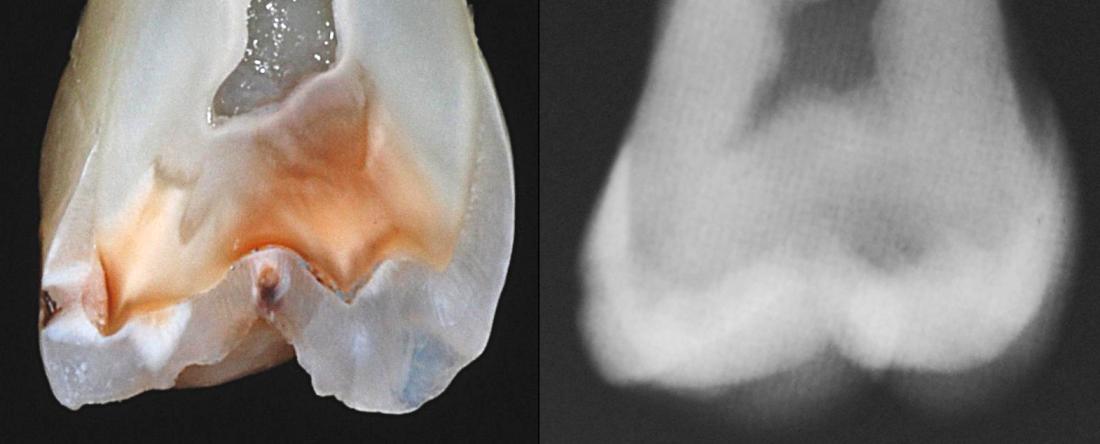 |
| Minimal mesial caries, picked up well on radiograph | 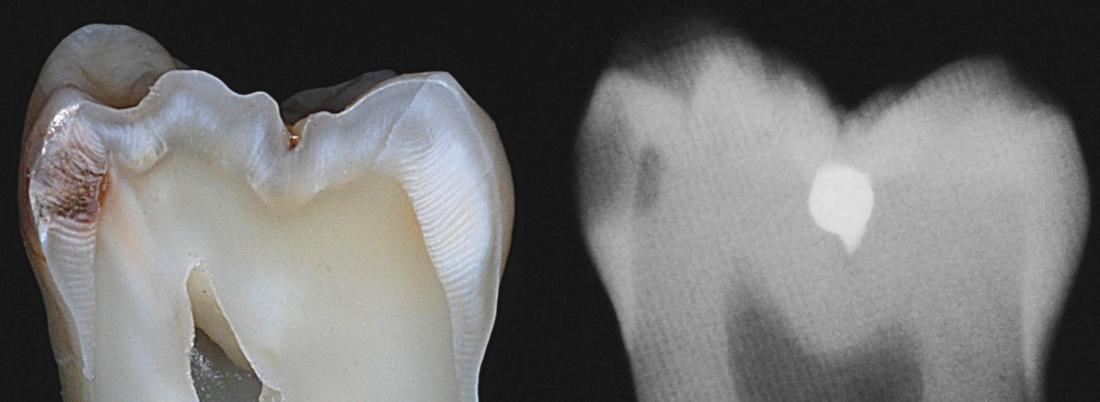 |
| Rapidly advancing fissure caries, young patient | 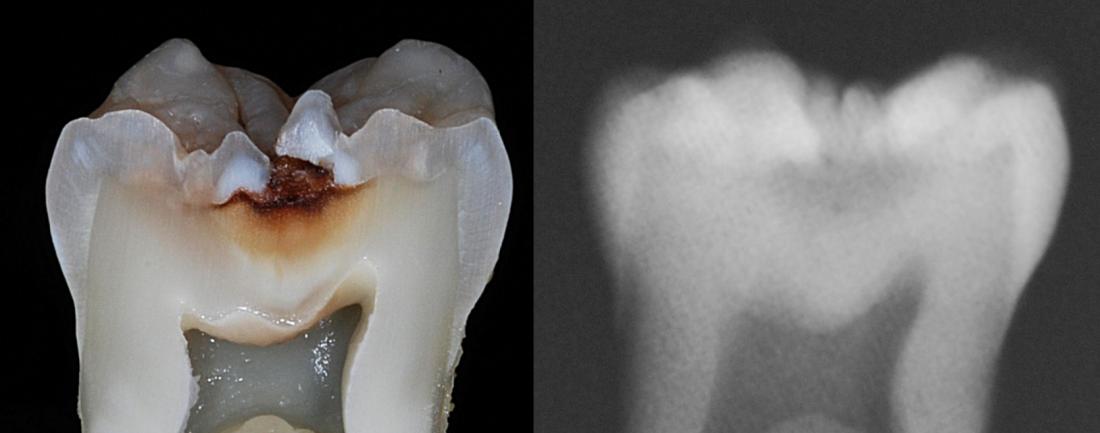 |
| Very early caries | 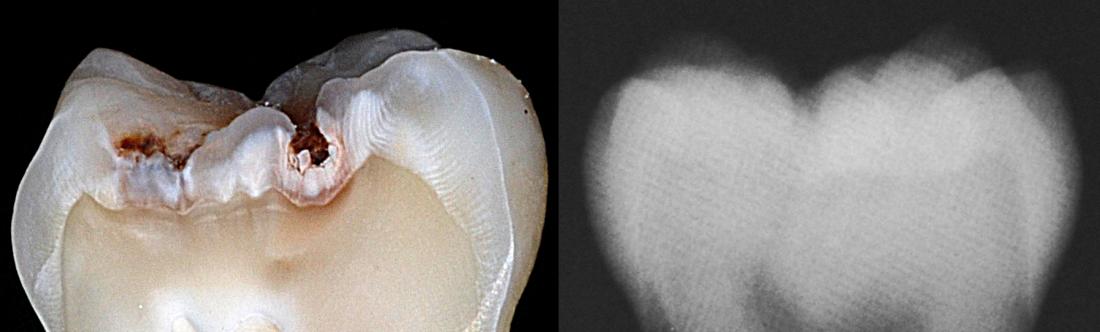 |
| Elderly patient | 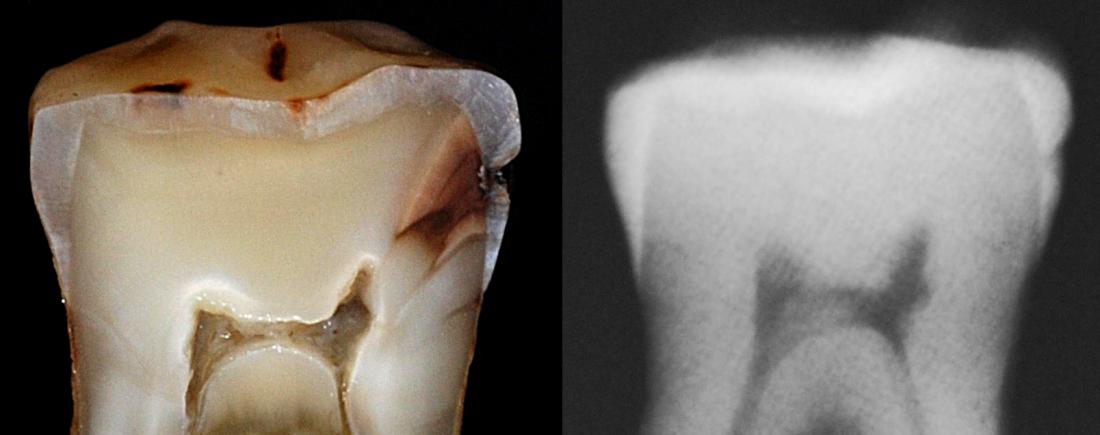 |
| Looks like it was cervical burnout? | 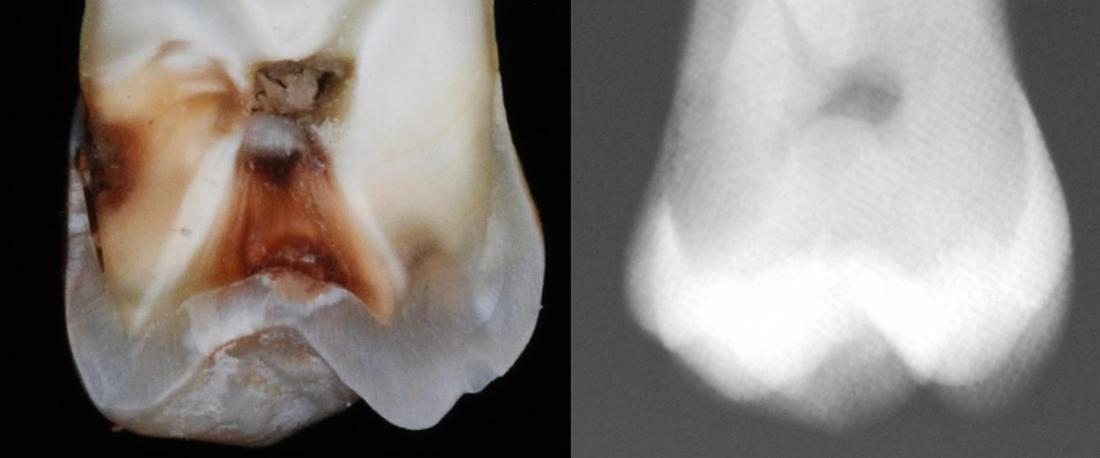 |
We hope you have enjoyed this "clinical" look at caries pathology. Radiographs can show the presence of caries, but can be unhelpful for establishing its extent, and whether or not operative intervention is needed. Also, they may not show caries when it in fact exists.
When there is doubt interproximally, always inspect the region for cavitation with a (contra-angled) probe first. Other aids to diagnosis include direct vision on the dried tooth, and electronic caries indicating devices like the Diagnodent.