Endodontics
Pulp Capping
Pulp capping is an operative technique designed to preserve the vitality of a potentially infected pulp. There are two broad types of pulp capping - the direct and the indirect pulp caps. They are only successful if the pulpal infection is very mild
We have put this topic into the endo section as, if you take the biological viewpoint for endodontology (study of the pulp in health and disease), we believe it belongs here more than in the "restorations" section.
The exposed pulp is directly covered. This works best when the exposure is not infected - for example a traumatic exposure caused by slipping with the drill.
If the pulp becomes exposed while removing soft infected dentine, the chances are that the pulp will be infected also, and a direct pulp cap will fail (that is, an irreversible pulpitis will develop).
Although Calcium Hydroxide has been proven successful for many years, MTA (Mineral Trioxide Aggregate) is fast becoming the material of choice for direct pulp caps. MTA is however very expensive.
The pulp is not exposed - a layer of infected dentine is deliberately left, rather than expose the pulp.
Indirect pulp caps, when done correctly, are more successful at maintaining long-term vitality than direct ones.
Procedure for "stepwise" indirect pulp cap

LR7 (47) Pre-op Radiograph. Advanced mesial (smooth surface) caries is present, and there is also a shadow that suggests occlusal (fissure) caries. This tooth was sensitive to cold stimuli, but did not hurt spontaneously.
A radiograph like this suggests that there is a high risk of pulpal exposure during preparation.
What precaution should be taken?
What does "aseptic" mean?
Remove caries until close to pulp, but not exposed. The radiograph is some help here, as it gives an idea of where the pulp horn is in relation to the caries.
How accurate is the radiograph in showing the extent of these features?

Place Calcium Hydroxide lining.
Primary teeth pulps are large, with extensive horns. The whole pulp floor should be covered, leaving just a small margin in the proximal box floor for the temporary restoration to seal. (This is unlike adult teeth, where just the smallest bit of Ca(OH)2 is placed in the deepest part.)
Why place a calcium hydroxide lining?
Could you use MTA instead of calcium hydroxide?
The lining is then covered with a tough temporary restoration, like glass ionomer or resin modified glass ionomer.
Note: It is not currently clear whether it is necessary to "go back in", but the trend is against this. Returning for more caries removal is called the Stepwise Technique, as the caries is removed in two steps separated by a couple of months. A paper by Maltz et al suggests that with permanent molars, after 3 years, no benefit is apparent.
Softened dentine may remineralise if gross infection is removed and the cavity can be sealed.
Next visit, at least 2 or 3 months later, remove the dressing.
Why 2 or 3 months? Why not wait much longer?
Final excavation performed. If hard dentine has formed, remove the last layer of caries.
What should you do if you expose the pulp while removing soft caries?
Place a new lining
This will stimulate further tertiary dentine formation.
Place a RMGI base over it.
What is the advantage of glass ionomer here?

Restore the tooth.
What monitoring would you undertake in the years to come?
Procedure for Direct Pulp Cap
 |
LRE pre-op radiograph |
 |
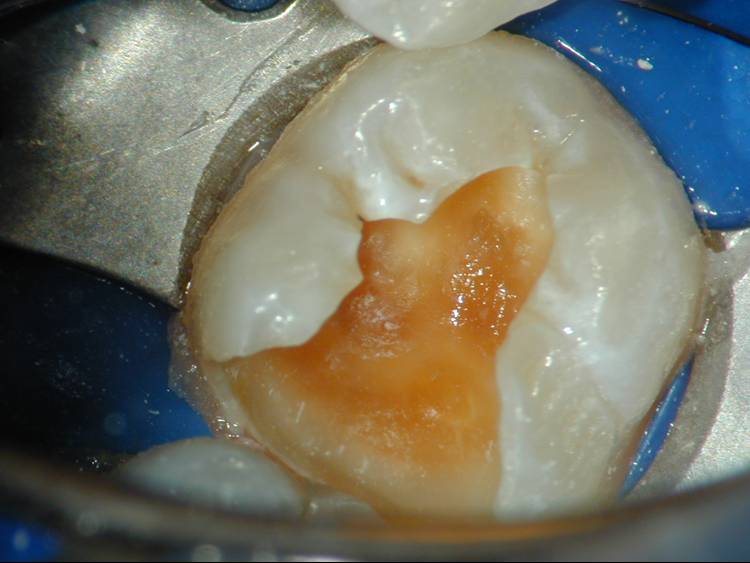
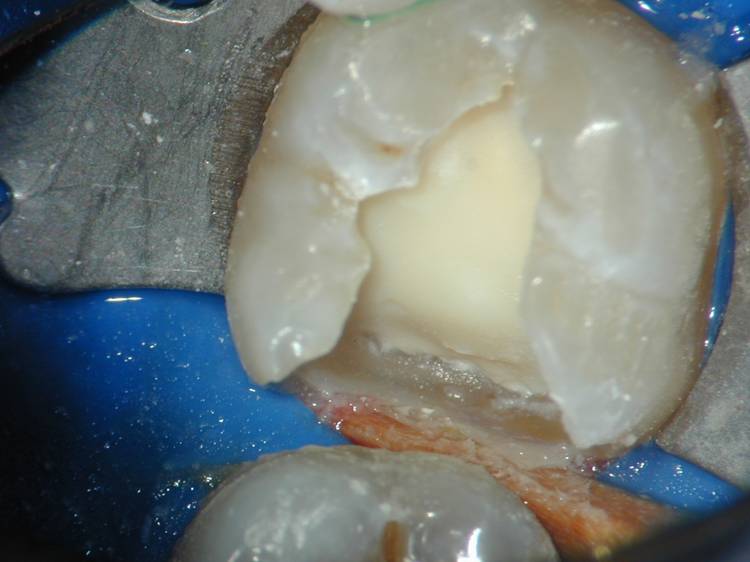
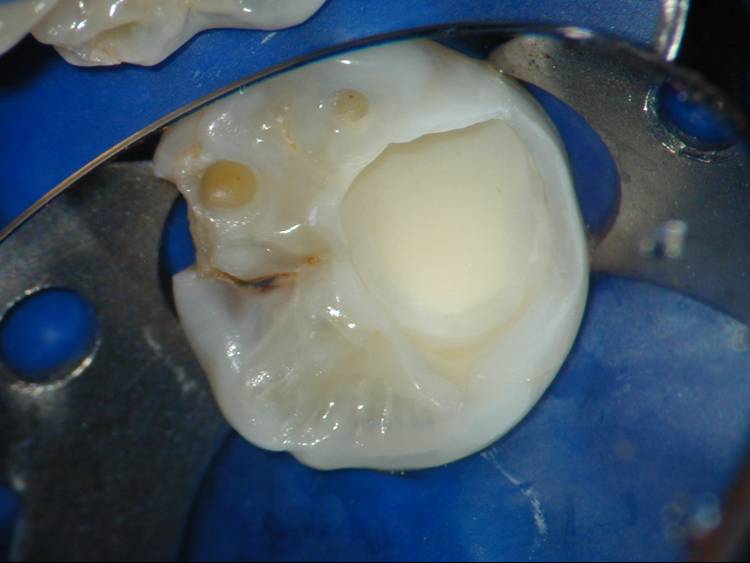
Exposed pulp. Can you see where? |
 |
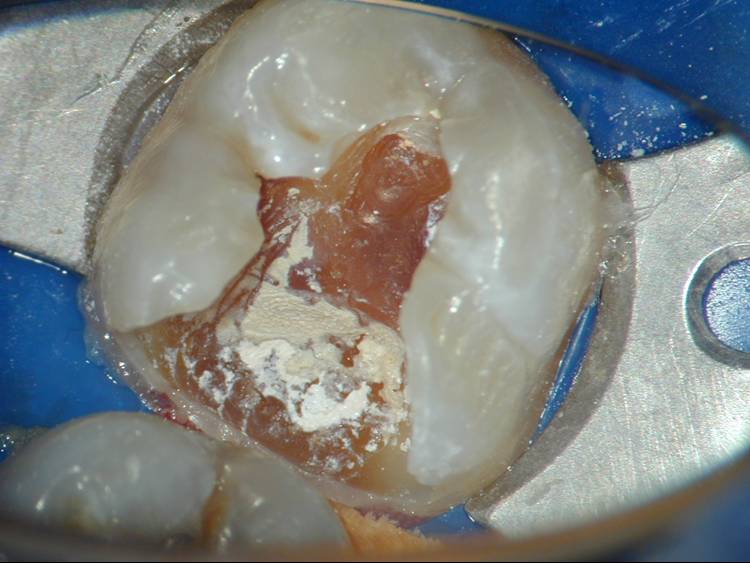
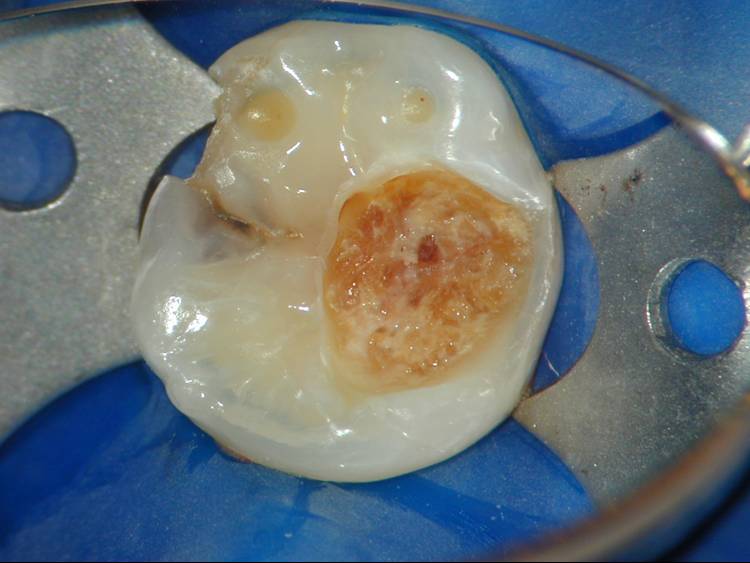
Continue caries removal. |
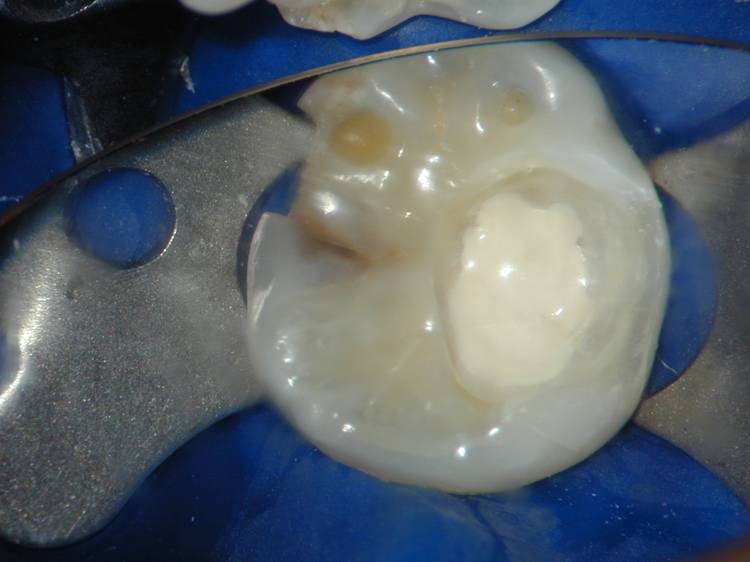 |
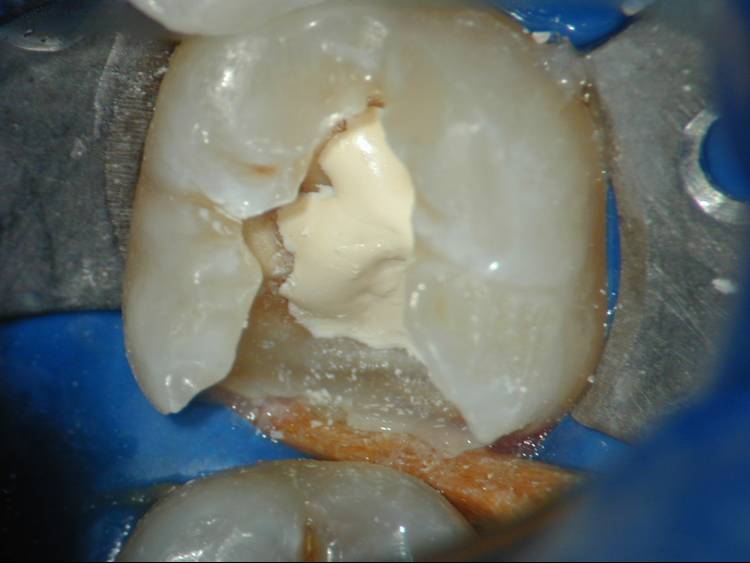
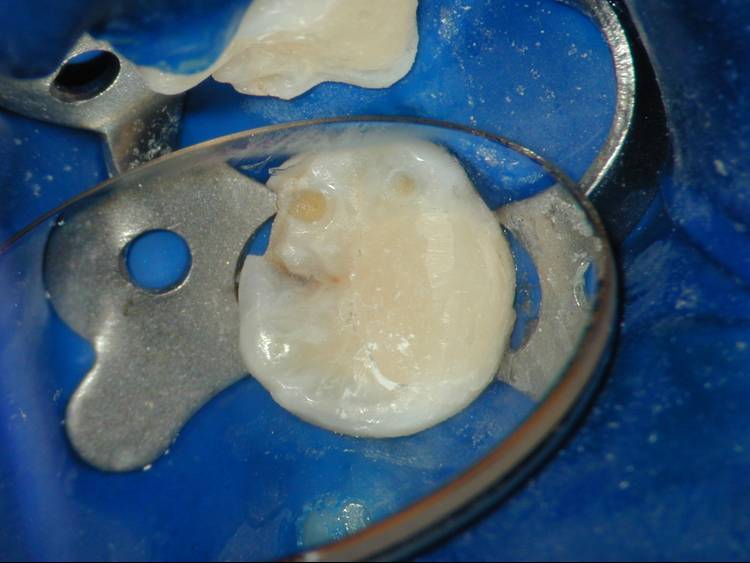
Place Calcium Hydroxide - direct pulp cap |
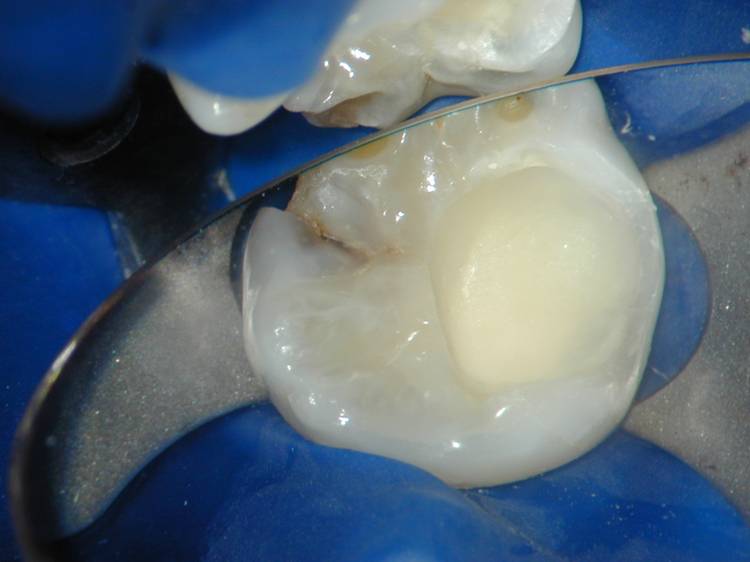 |
Place RMGI lining |
 |
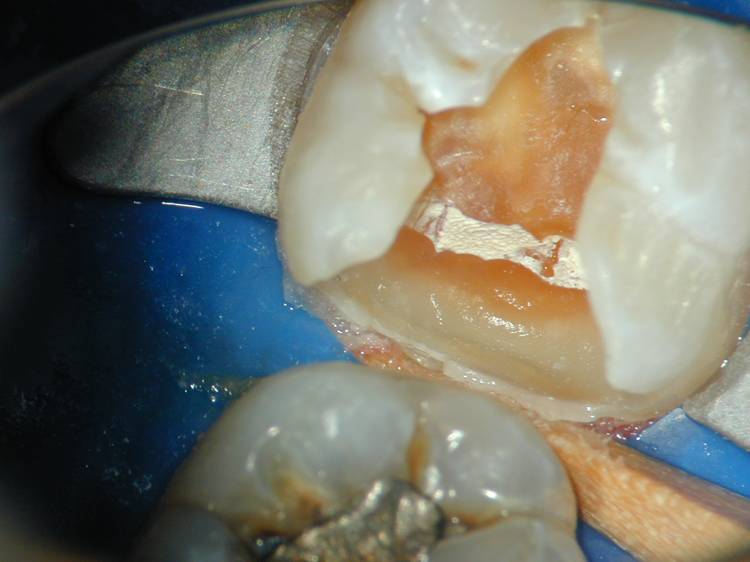
Etch |
 |
Check frosted appearance after etch |
 |
Restore. Seal remining fissure caries. |
|
Follow up regularly to ensure vitality maintained. RCT (probably pulpotomy for a deciduous tooth) or extract if not. The key factor in pulpal healing after exposure is absence of infection ~ Calcium Hydroxide is antibacterial. |
|